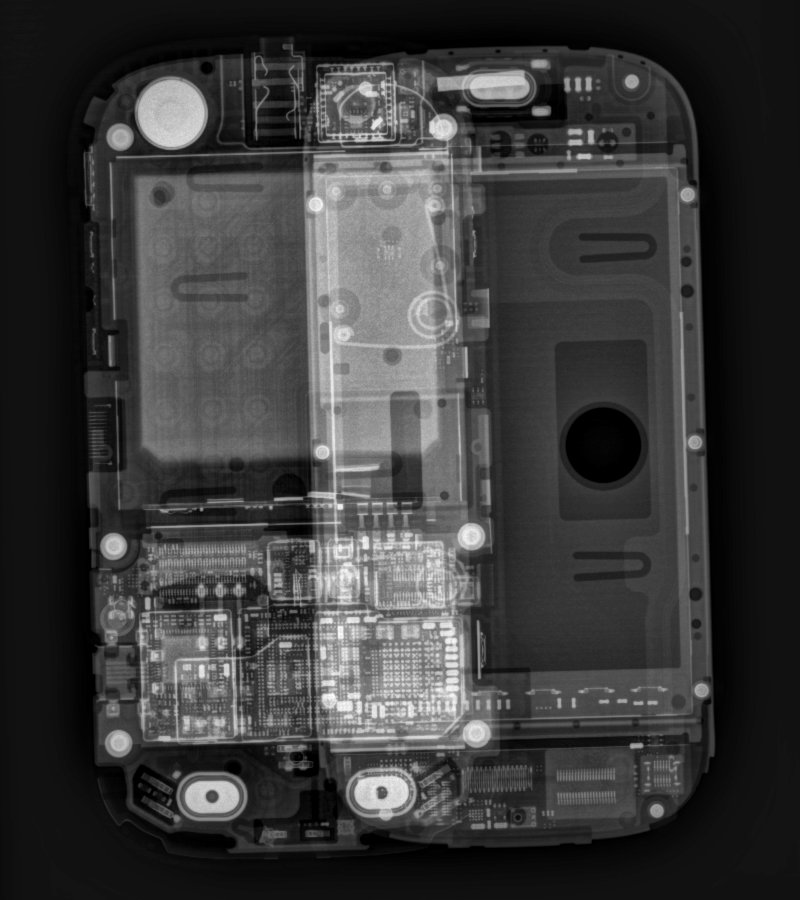
I was doing some testing on a radiographic room today and took the opportunity to get a better x-ray image of my Galaxy S II. This was acquired using 80 kV, 5 mAs with a little bit of magnification.

Compared to the previous x-ray I took, the NFC antenna integrated into the battery looks like it’s probably the series of concentric traces, like those RFID security tags you find in books and stuff. The components on the circuit boards are also much more visible in this one.
Galaxy S II X-ray
A new Orthoscan mini C-arm arrived at the hospital last week, so while I was doing the acceptance testing on it today I used it to get a shot of my Galaxy S II.

The big grey blob in the middle is the battery and the vertical stripe in the battery I’m guessing is the NFC antenna. The square just below the top would be the camera. The square to the left of that just below the top is the front facing camera. On the right side is the headphone jack. The rectangular thing at the bottom to the right of the USB/HDMI connector is the speaker I think.
Cliq in X-ray
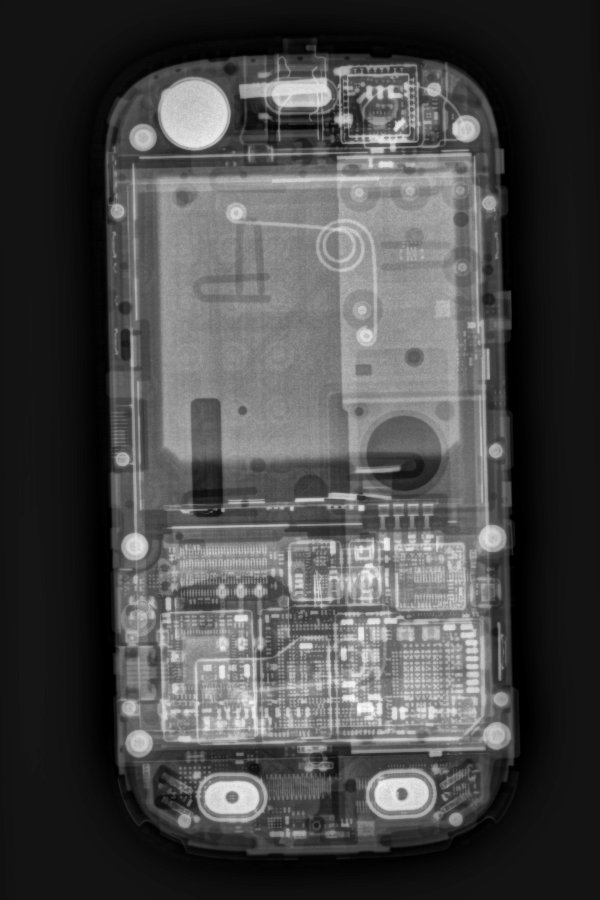
81 kVp, 2.6 mAs, small focal spot
111 years of x-rays
111 years ago today, a physicist by the name of Wilhelm Röntgen caught a glimmer of light coming from a fluorescent screen located across the room from his cathode ray tube setup. The strange phenomenon caught his interest and he spent several weeks investigating the matter.
Röntgen had just “discovered” x-rays. A month later he created the first radiograph (röntgenograms as they were called back then), an x-ray image of his wife’s hand. The new rays were a huge hit among physicists, enabling the discovery of all kinds of wonderful things about the properties of matter. Once word reached the medical community of this new discovery, it wasn’t long before Röntgen’s new rays were used to image and treat patients.
The first x-rays were used to treat a breast cancer patient a mere two months after Röntgen’s discovery. Shortly after came Edison’s fluoroscope machines for visualizing x-rays in real-time. From there, the rest was history.
References:
Juan A del Regato, Radiological Physicists, American Association of Physicists in Medicine, 1985
Seliger HH, “Wilhelm Conrad Röntgen and the Glimmer of Light”, Physics Today, 1995(11), 25-31
Review: NCRP 147 – Structural Shielding Design for Medical X-ray Imaging Facilities
Amazon’s review system apparently wasn’t working when I tried to submit this there, so I’ll put it here instead (I probably would have put it here anyway).
A few months ago, I unexpectedly received a fat FedEx envelope containing a draft copy of the much anticipated rewrite of NCRP 49: Structural Shielding Design and Evaluation for Medical Use of X-Rays and Gamma Rays of Energies Up to 10 MeV. Turned out it came to me because I’m on the AAPM Diagnostic Imaging Committee, and committee members were asked to review the draft to make sure there weren’t any glaring errors or anything. Sweet, so I dug in. Been hearing about this thing for years, and was eagerly awaiting it’s completion, like many other medical physicists out there.
A few weeks ago, I was rewarded for my efforts as a committee member reviewer by a surprise complimentary copy of the newly published NCRP 147. Even sweeter. And a hardcopy version to boot.
NCRP Report 147: Structural Shielding Design for Medical X-Ray Imaging Facilities
This is an invaluable upgrade to NCRP 49, and probably needs to be added to the collection of every medical imaging physicist that does shielding calculations. The focus is on shielding for imaging rooms, so there is much more relevant content for imaging physicists than there was in NCRP 49 which covered imaging and therapy shielding. New methods and techniques have been introduced which results in somewhat less conservative shielding requirements than what would have been required under the ultraconservative NCRP 49. Chapter 5 provides sample shielding calculations for just about every type of imaging room there is. This is a well written and much needed update to the original NCRP 49.
Even though I’ve already been through the draft, I’m going through it again, because this is the kind of thing medical physicists need to know like the back of their hand. Much of the content and calculations are similar to what was in NCRP 49, but there are enough new things in the rewrite that makes it worth studying thoroughly.